

Balls, Sockets, SLAPs, and Taps – reliable, evidence-based exam maneuvers to illuminate the Glenoid Cavity
Big shout-out to G.G. this week who SLAPped together a last-minute Teaching Tuesday session on the shoulder AND tricked had Sports Medicine Specialist Dr. John Touhy join in!
The first Clinical Pearl – check your eponyms at the door. That’s right. It turns out that the mile-long list of eponymous PEX maneuvers you memorized during Medical School does very little to bolster your diagnostic acumen when you see that next Weekend Warrior.

Enter JAMA’s Rational Clinical Exam series and its Meta-Analysis identifying the PEX maneuvers that YOU can actually use in REAL LIFE toaccurately diagnose the MOST COMMON CAUSE OF shoulder pain – Rotator Cuff Disease (RCD). Shoulder Pain and Rotator Cuff Disease
The Bottom Line – Only TWO PEX findings reliably identify RCD … and neither Neers nor Hawkins make the cut.
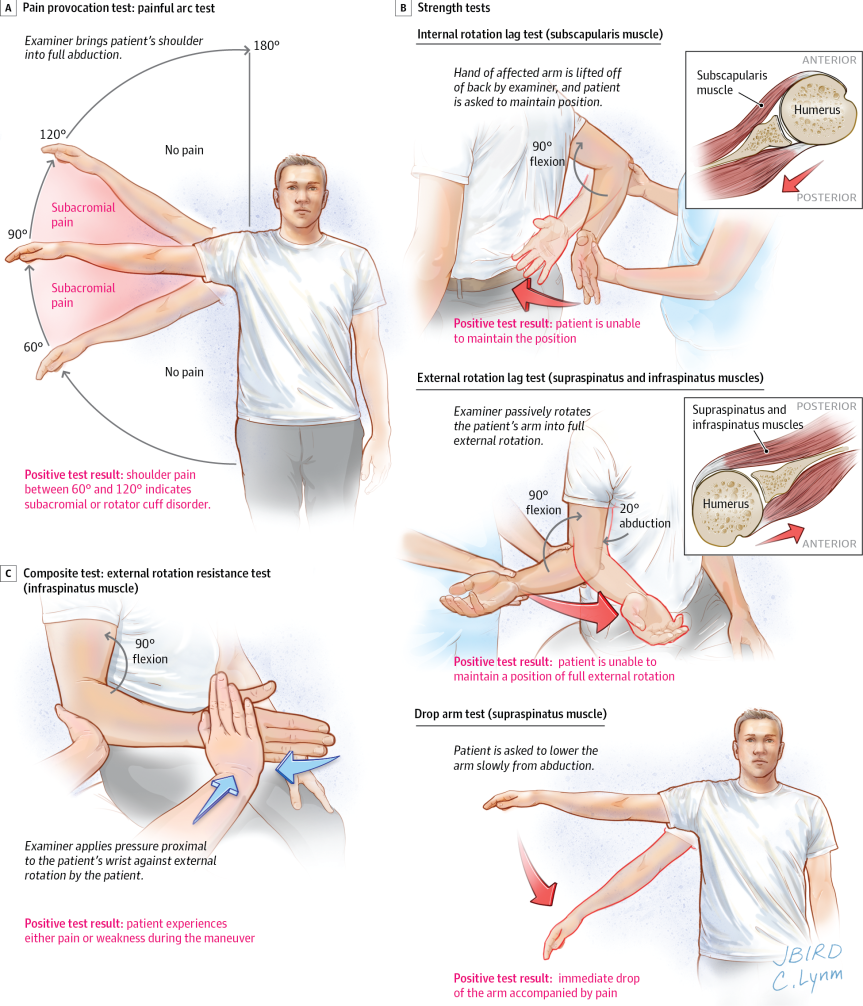
- A positive painful arc test result was the only finding with a positive LR greater than 2.0 for RCD (3.7 [95% CI, 1.9-7.0]), and a normal painful arc test result had the lowest negative LR (0.36 [95% CI, 0.23-0.54a positive external rotation lag test (LR, 7.2 [95% CI, 1.7-31]) and internal rotation lag test (LR, 5.6 [95% CI, 2.6-12]) were the most accurate findings for full-thickness tears]) – among pain provocation tests
- A positive external rotation lag test (LR, 7.2 [95% CI, 1.7-31]) and internal rotation lag test (LR, 5.6 [95% CI, 2.6-12]) were the most accurate findings for full-thickness tears – among strength tests.


